- Plastic Surgery
Malar Edema and Festoons: Differences, Causes, and Modern Treatment
- April 12, 2026
- By Fernando Amato
Malar edema and festoons are aesthetic changes in the area below the eyes that often cause confusion for both patients and professionals. Although they may appear similar at first glance, they have different origins and often coexist in the same patient. This overlap thus makes diagnosis and treatment more challenging — and requires a careful, individualized approach based on multiple anatomical levels.
In this article, you will understand what these conditions are, why they arise, how to differentiate one from the other, and what the most modern treatment options are, including surgical and non-surgical approaches.
What is malar edema
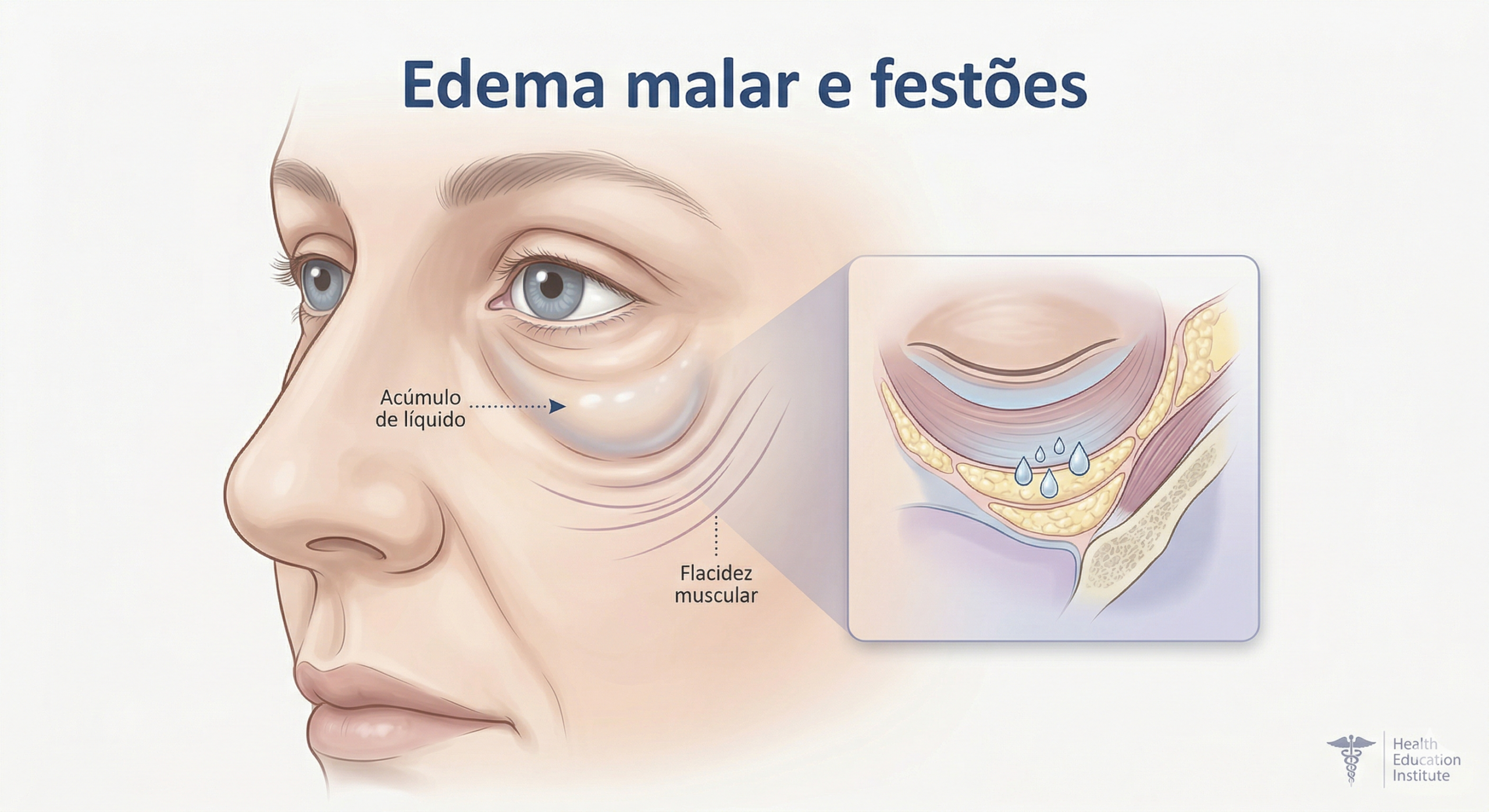
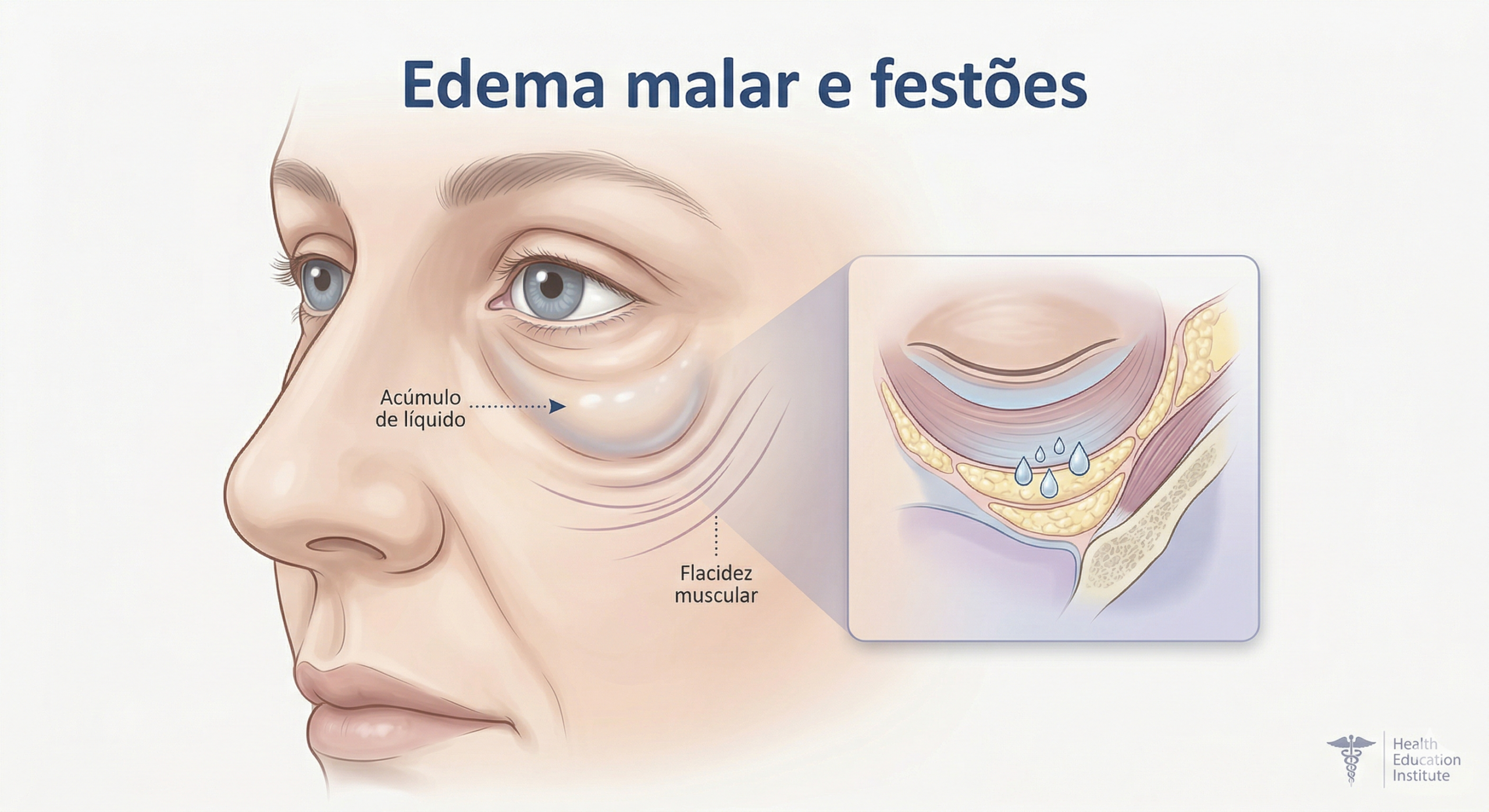
Malar edema, also called “malar mound,” is an accumulation of fluid and/or tissue in the cheekbone area, just below the lower eyelid. It can give the impression of persistent swelling, even in young people.
Therefore, from a technical point of view, it is an alteration in lymphatic drainage and fluid retention in a specific compartment of the face. In simple terms, it is as if the body has difficulty “draining” fluids from that region.
Among the main associated factors are:
- Aging of the skin and deep tissues
- Muscle laxity
- Changes in lymphatic drainage
- Prior use of facial fillers
- Genetics
What are festoons
Festoons are more evident and structured folds in the area below the eyes, usually appearing as more pronounced and heavy bags. Unlike malar edema, they involve not only fluid but also lax skin and muscle.
In technical terms, however, there is redundancy (excess) of skin and relaxation of the orbicularis oculi muscle — the muscle that surrounds the eyelid.
In practice, festoons usually:
- Are more visible when smiling
- Have the appearance of “sagging bags”
- Persist even with rest
Why it is difficult to differentiate malar edema and festoons
In most patients, there is no clear separation between these two conditions. It is common to have a combination of:
- Fluid accumulation (edema)
- Muscle laxity
- Excess skin
Therefore, many specialists choose to treat both integratively, rather than trying to classify them rigidly. This modern view avoids incomplete treatments and improves results.
Main causes — with emphasis on fillers
One of the most relevant changes in recent years has thus been the increase in cases related to the use of hyaluronic acid fillers.
Although widely used and safe when properly indicated, these products can cause:
- Fluid retention in the malar region
- Compression of lymphatic channels
- Irregularities in facial contour
Today, many specialists consider fillers the most common cause of acquired malar edema.
When this occurs, the approach may thus include the application of hyaluronidase — an enzyme that dissolves the product — before any surgical approach.
Evaluation before treatment
Before defining the treatment, a complete evaluation is essential, which may include:
- Analysis of skin quality
- Degree of muscle laxity
- History of aesthetic procedures
- Presence of fillers or fat grafting
This step is as important as the treatment itself. In fact, detailed pre-operative exams are fundamental, as explained in pre-operative exams
Non-surgical treatments
Not all cases require surgery. In mild or initial situations, some options can help:
- Lymphatic drainage
- CO₂ laser for skin improvement
- Dissolution of fillers with hyaluronidase
- Specific adjustments with deep filling (in specific cases)
However, these methods have limitations. When there is structural laxity, the result tends to be partial.
Modern surgical treatment of malar edema and festoons
In moderate to advanced cases, a surgical approach usually offers more consistent results.
One of the most comprehensive techniques involves a combination of procedures that act on different layers of the face.
Deep-plane rhytidectomy (facelift)
Modern rhytidectomy does not only treat the skin. It also acts on the SMAS (Superficial Musculoaponeurotic System), a deep layer responsible for facial support.
By repositioning this structure, it is possible to:
- Improve the transition between eyelid and cheek
- Reduce the “heavy” appearance of the face
- Soften festoons and malar edema
This concept also appears in other facial contouring procedures, such as mammoplasty and mastopexy, where structural support is essential for lasting results.
Orbicularis oculi sling
One of the most important techniques is the “orbicularis sling.”
It involves a suspension of the muscle around the eyes, which is lifted and fixed in a higher position.
Benefits include:
- Improved lower eyelid support
- Reduction of muscle laxity
- More harmonious contour of the region
This technique can be performed during blepharoplasty or even alone in selected cases.
Canthopexy and eyelid support
Canthopexy is a procedure that reinforces the lateral corner of the eye (outer region of the eyelid).
It is especially important to prevent complications such as:
- Ectropion (eyelid turned outward)
- “Scleral show” (excessive exposure of the white part of the eye)
In higher-risk patients, additional measures may be used, such as:
- Temporary tarsorrhaphy
- Frost suture
These techniques help protect the eyelid in the postoperative period.
Importance of anesthesia and surgical environment
The safety of the procedure also depends on factors such as adequate anesthesia and hospital structure.
Learn more about these aspects in anesthesia and day hospital
Possible complications
Like any surgery, there are risks that should be considered:
- Prolonged edema
- Asymmetry
- Ectropion
- Visible scars (rare with modern techniques)
Therefore, choosing a qualified professional and proper follow-up are fundamental.
Care before and after surgery
Proper preparation significantly improves results.
Before surgery:
- Avoid smoking, as advised in smoking risks
- Follow dietary guidelines, as in diet
- Undergo all requested examinations
After surgery:
- Maintain relative rest
- Avoid sun exposure
- Follow medical instructions correctly
See general guidelines in tips for preparing.
What about fat grafting?
Fat grafting can be useful in some cases, but it should be done with caution.
When performed in excess, it can cause:
- Irregularities
- Nodules
- Increased malar edema
The current trend is to be conservative, avoiding “overcorrection.”
Direct excision of festoons
In selected cases, especially when festoons are well-defined, direct removal can be considered.
This approach is more direct but requires experience to avoid visible scars.
What the medical literature says
Studies show that the most effective treatment generally involves a combined approach — skin, muscle, and deep structures.
A review available in PubMed highlights that techniques that reposition the SMAS and thus reinforce muscular support tend to present more lasting and natural results.
Conclusion
In summary, malar edema and festoons are complex conditions that often coexist and require an individualized approach.
However, modern treatment goes beyond the skin, acting on multiple levels of the face to restore natural support and contour.
Thus, the choice of technique depends on several factors, and an evaluation with an experienced plastic surgeon is indispensable to define the best strategy.
FAQ
What is malar edema?
It is an accumulation of fluid in the cheekbone area, below the eyes.
Are festoons the same as eye bags?
Not exactly. Festoons involve lax skin and muscle, while bags can be just fat.
Can filler cause malar edema?
Yes. Hyaluronic acid can interfere with lymphatic drainage and cause persistent swelling.
Does all malar edema require surgery?
No. Mild cases can be treated with non-surgical measures.
What is the orbicularis muscle sling?
It is a technique that repositions the muscle around the eyes to improve eyelid support.
Does the surgery leave a scar?
Scars are generally discreet and well-positioned.
How long do the results last?
It depends on the technique and the patient, but structural procedures tend to last longer.
Is it possible to treat only with laser?
Laser helps with skin but does not resolve significant muscle laxity.
What is ectropion?
It is when the lower eyelid turns outward.
How to know which treatment is ideal?
An evaluation with a specialist is essential to define the best approach.
Related articles



Agendar consulta
Precisa de orientação personalizada?
Marque uma avaliação com o Dr. Fernando Amato e tire as suas dúvidas sobre cirurgia plástica.
Falar no WhatsApp